Today’s Date:
First Name
Last Name
Date of Birth
Social Security Number
Preferred Provider
Email
Marital Status
Occupation
Address
City
State
Zip
County
Home/Cell:
Work Phone
Primary
Pharmacy Name
Pharmacy Address
Race
Ethnicity
Preferred Language
Country of Origin
Emergency Contact
Relationship to Patient
Patient ID
Primary Insurance Company Name
Street Address
Subscriber Info/Member ID
Group #
Insurance Start Date
Subscriber Info
Sex
D.O.B
Patient Relationship to Subscriber
Subscriber SSN
Secondary Insurance Company Name
Yes, to facilitate the communication of tests results and other information; I authorize Associates in Women's Health to use my Voicemail if the physicians and staff are unable reach me directly.(Please check the phone number that you would like us to use.)
No, I do not authorize Associates in Women's Health to leave confidential information(tests results) on my Voicemail.
Home Phone
Cell Phone
SIGNATURE
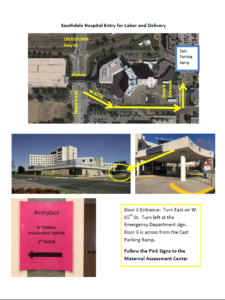
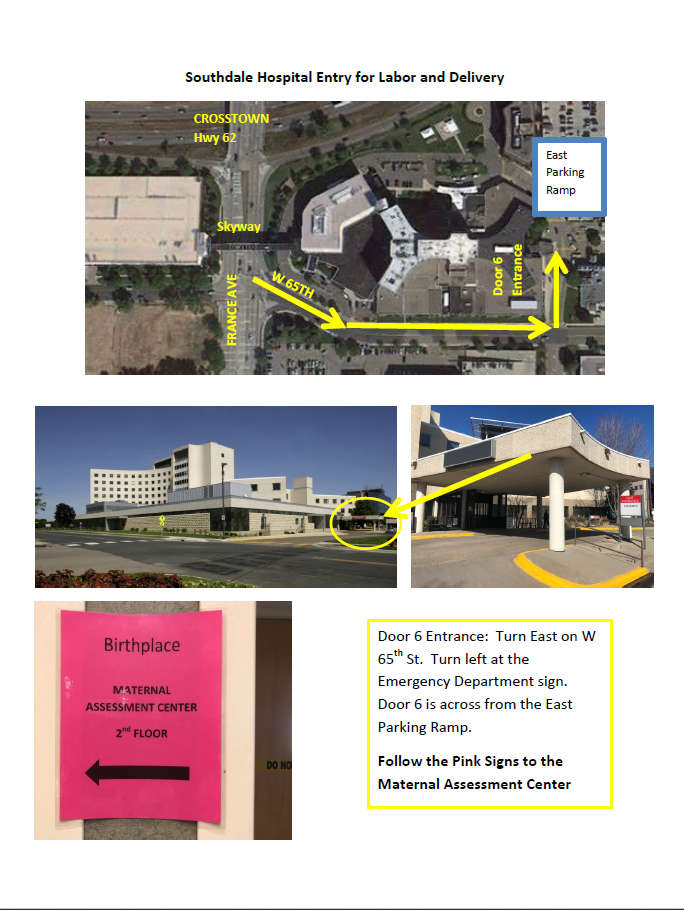
Directions to Southdale Hospital for Labor and Delivery
Map to Southdale Hospital Labor and Delivery