Name
Relationship
HEALTH NETWORK SHARING: Your physician would like to ensure that you receive the best possible care. It is important to coordinate care amongst your primary care providers here and providers who may care for you elsewhere. When you give permission to your insurance plan to share that information with us, you help to ensure that the providers are able to care for you in the most cost effective and efficient way possible.My insurer may share my past, current and future health and account records with Associates in Women's Health about services I’ve received from Associates in Women's Health and other care providers unrelated to Associates in Women's Health. These records may be used by Associates in Women's Health as needed to manage or coordinate my care and to improve the quality of that care.
If I DO NOT agree to this, I will initial here_______________________. My insurer may not release any of my identifiable health records from providers unrelated to AWH for the purposes described above.
Patient Name
Date of Birth
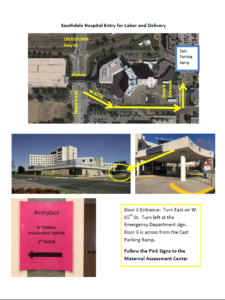
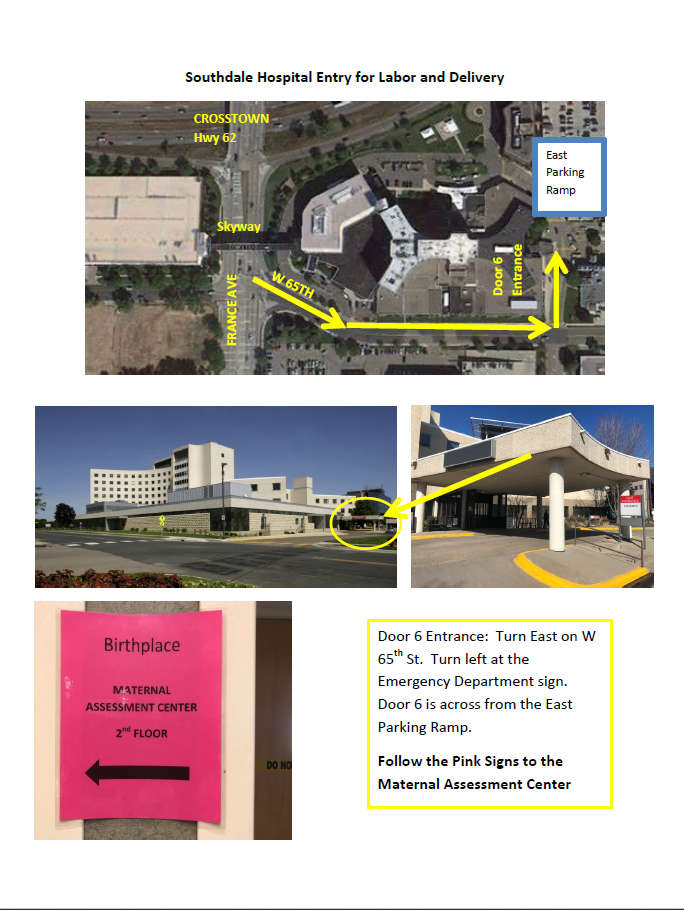
Directions to Southdale Hospital for Labor and Delivery
Map to Southdale Hospital Labor and Delivery