Date
Name:
Preferred Name:
DOB:
Primary Care MD/Clinic:
Referring MD:
Medication Allergies/Reactions:
None
Eggs
Latex
Iodine
Current Contraception (including tubal ligation, vasectomy, condoms, etc.)
Date of last annual exam:
First day of last menstrual period:
What symptoms and concerns do you want to discuss?
Have you seen another provider for the same condition?
No
Yes
Pap Smear:
Please list date of last pap smear
Date/Treatment
Normal
Abnormal
Mammogram:
Please list date of last mammogram
Never
Colonoscopy:
Please list date of last colonoscopy
Bone Density:
Please list date of last bone density
Age at Onset (your first period):
Frequency:
Days of Flow:
Heavy Flow
Bleeding Between Periods
Bleeding After Intercourse
Menstrual Cramping
PMS
Menopause (age):
Surgical Menopause (date):
No changes since last completed form
#Partners in Last Year
#Lifetime Partners
Male
Female
Both
Does anything listed apply to you:
Urine:
Frequency
Urgency
Burning
Incontinence
Pain
Vagina:
Dryness
Itching
Discharge
Painful Intercourse
Menopause:
Hot Flashes
Night Sweats
Bleeding
Other
Other:
AIDS/HIV
Chlamydia/Gonorrhea
Genital Warts
Herpes
Marital Status
Single
Married
Divorced
Widowed
Separated
Are you employed?
Is anyone physically, sexually, or emotionally hurting you?
Do you wear seat belts?
Do you have carbon monoxide indicators in your home?
Do you have smoke detectors in your home?
Do you use tobacco/e-cig?
Drink alcohol?
Do you use street drugs?
Exercise
Routine of
Special diet
Weight Loss
Low Fat
Vegan
Diabetic
Vegetarian
Low Carb
Do you drink caffeinated beverages?
Quantity/Frequency
Constitutional
Anorexia/Bulimia
Weight Gain
Fatigue
Sweating
Eyes
Double Vision
Spots
Vision Loss
Ear/Nose/Throat
Ringing in Ear
Earache
Sore Throat
Bleeding Gums
Congestion
Cardiac
Chest Pain
Palpitations
Swelling/Edema (location)
Respiratory
Wheezing
Cough
Shortness of Breath
GI:
Constipation
Diarrhea
Bloating
Black or Bloody Stools
Muscle
Joint Pain
Muscle Cramps
Weakness
Skin
Rash
Lesions
Acne
Moles
Breast
Lump
Fibrocystic
Skin Changes
Neuro:
Headaches
Tremors
Seizures
Psych
Depression
Anxiety
Insomnia
Memory Loss
Moodiness
Endo
Excess Thirst
Hair Loss
Hair Growth
Cold/Heat Intolerance
Excess Urination
Lymph
Bruising
Nosebleeds
Swollen Glands
Have you experienced any of the following?
Asthma
Cancer
Stroke
Diabetes
Heart Disease
Ulcers
Thyroid Problems
Phlebitis
Arthritis
Diverticulitis
Kidney Infection
Gonorrhea/Chlamydia
Please include yourself, immediate family, grandparents, aunts and uncles
Have you had a TB test (mantoux)?
Year
Result
Do you have specific requests for
New Medication
Tests
Refills
Completion of forms
Vaccinations
School or work release
Referrals
Patient’s Signature
Thank you for taking the time to complete your medical history!
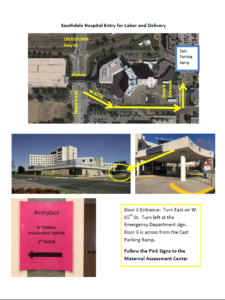
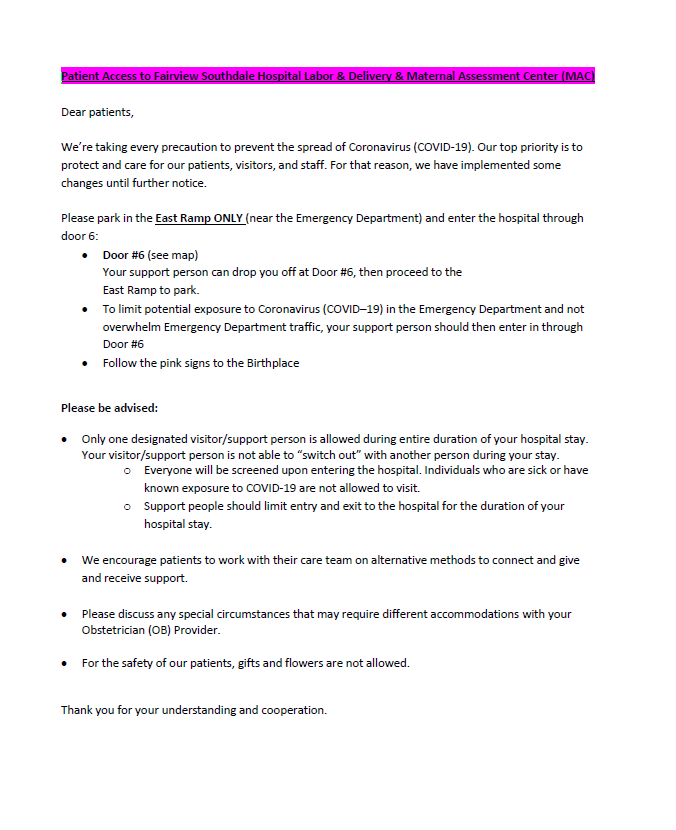
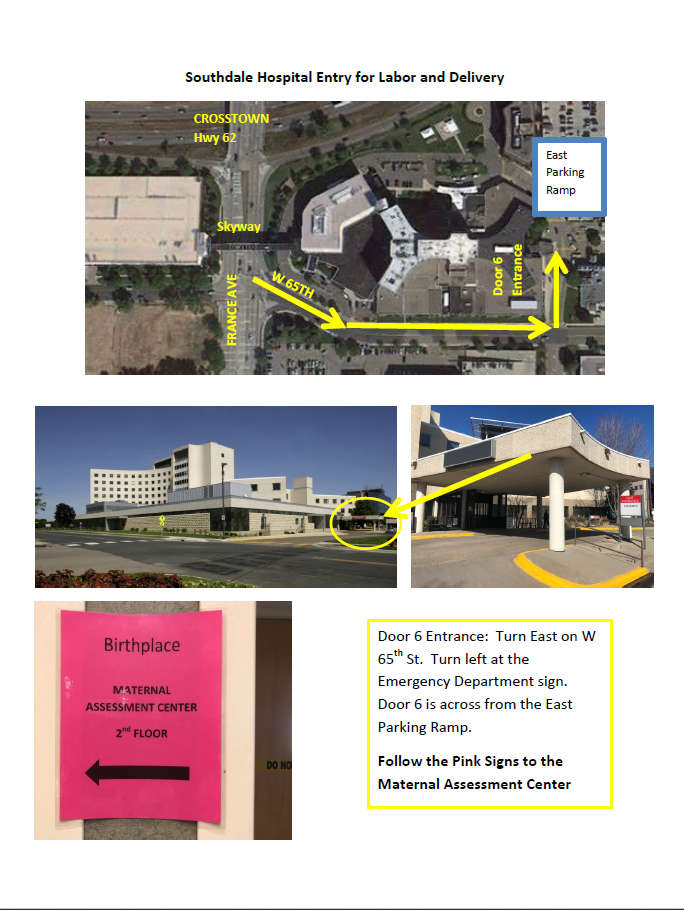
Directions to Southdale Hospital for Labor and Delivery
Map to Southdale Hospital Labor and Delivery